Demystifying our inflated calcium intake recommendations
Vegan Society of Canada News
Published January 23rd 2020
Updated February 5th 2026
Why We Updated This Article
Since our last update in 2024, several new studies have added important nuance to our understanding of calcium needs, supplementation risks, and long-term health outcomes. This emerging research highlights how factors such as sodium intake, overall dietary pattern, protein sources, and plant-food diversity influence calcium absorption and retention, and how these factors may contribute to differences in calcium requirements across populations.
Our mission remains the same: to present evidence grounded in high-quality, independent research; to reflect the best available global science; and to support Canadians in making informed, compassionate, and sustainable health decisions.
Growing evidence suggests that calcium needs may not be determined solely by meeting a single universal intake target, but are shaped by broader diet and lifestyle patterns that affect how efficiently calcium is used by the body. This review examines whether current intake goals are truly appropriate for everyone and how those who avoid animal-based foods may benefit from a more personalized approach to achieving sufficient calcium.
Why Calcium Matters
Calcium is still one of the body’s core structural and regulatory minerals. About 99% of all calcium is stored in the skeleton, acting as a long-term reservoir that the body taps into whenever dietary intake is insufficient. The remaining 1%, though small, is essential for nerve transmission, muscle contraction, blood clotting, enzyme activity, and hormone signalling. Tight regulation of calcium is essential to keep these systems functioning.
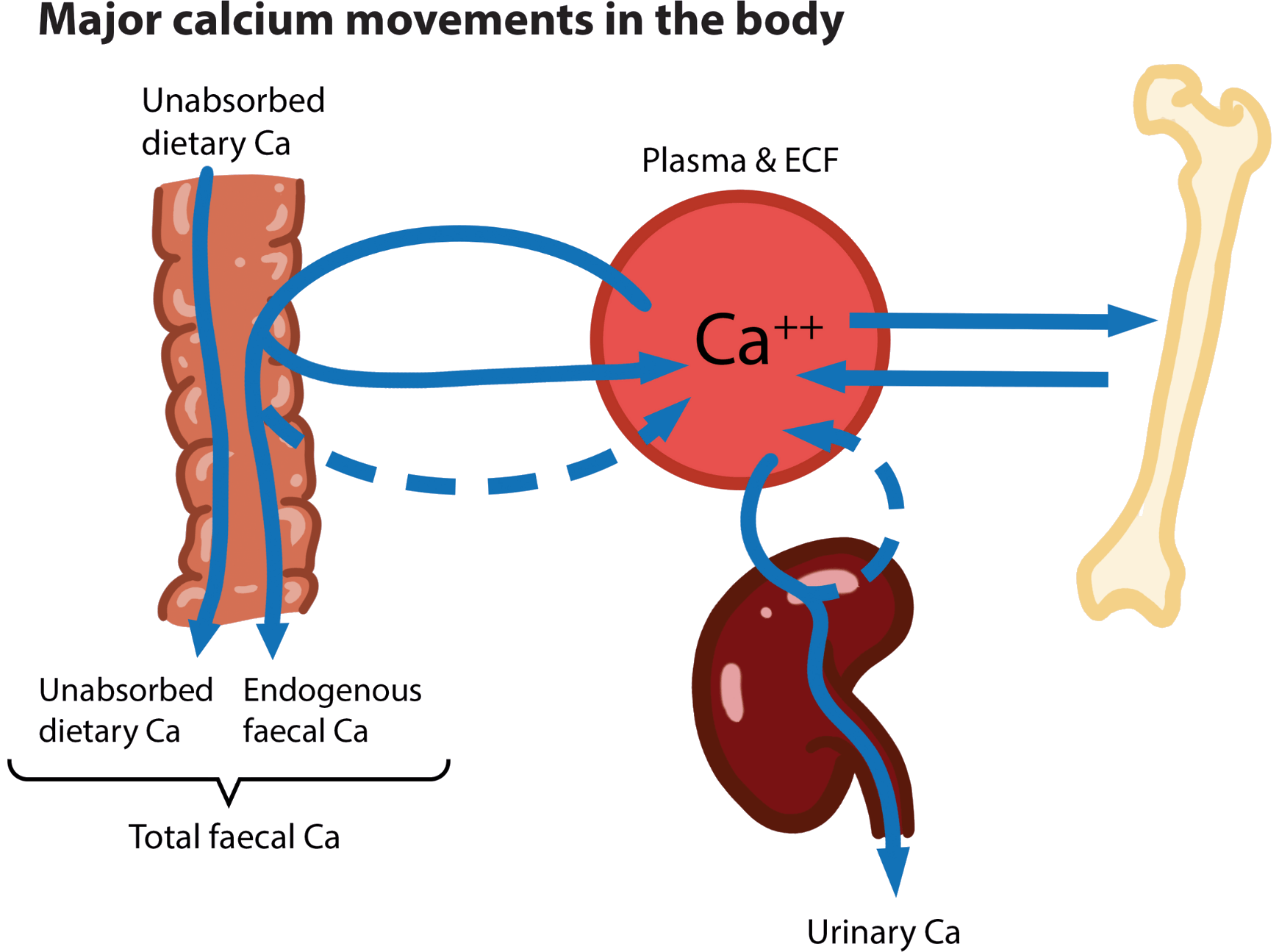
Calcium Balance: More Than How Much You Eat
Calcium status is a dynamic interplay between absorption and excretion. Positive balance stores calcium in bone, while negative balance draws from bone, gradually reducing bone mineral density. Recent evidence highlights that absorption and retention, not just intake, are key drivers of skeletal outcomes.
What Impacts Calcium Absorption and Loss?
Calcium absorption isn’t fixed. It shifts depending on many factors. Researchers often emphasize that absorption ranges widely (roughly 20–60% depending on context), so understanding the key factors can help you support your bones more effectively.
Universal factors
Diet
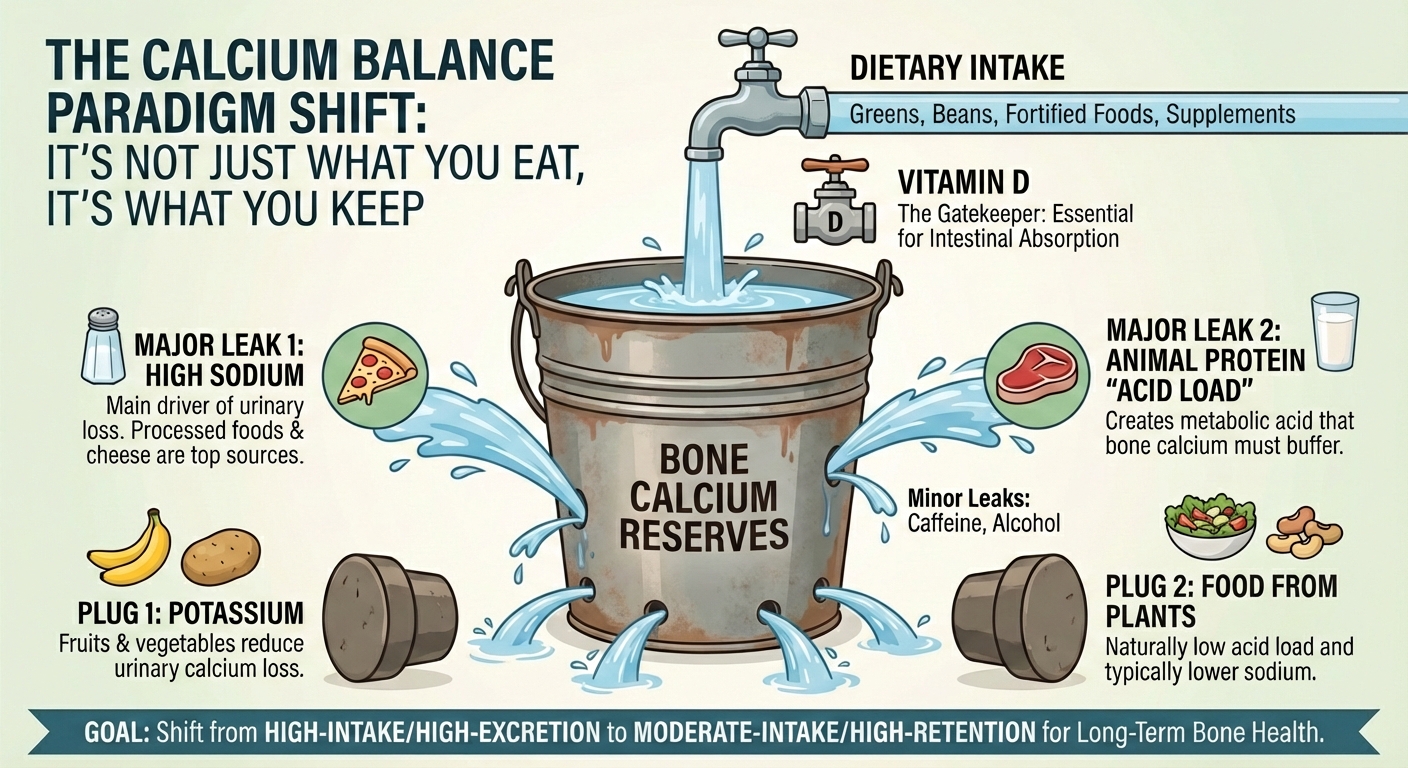
- High sodium intake is a major driver of urinary calcium excretion. In the standard Canadian diet, the leading sources of sodium are not the salt shaker, but processed foods, with cheese and dairy-heavy ultra-processed foods, such as pizza, ranking as top contributors. Thus, a high-dairy diet creates a physiological paradox: the consumer ingests calcium in cheese that simultaneously delivers the sodium required to flush that calcium out of the bones.
- High protein intake can elevate calcium excretion via acid-base balance effects.
- Low potassium intake elevates calcium excretion. A study found that increasing potassium intake by roughly 1,000 mg/day (from fruits and vegetables) reduced urinary calcium excretion by about 14 to 20 mg/day in healthy adults.
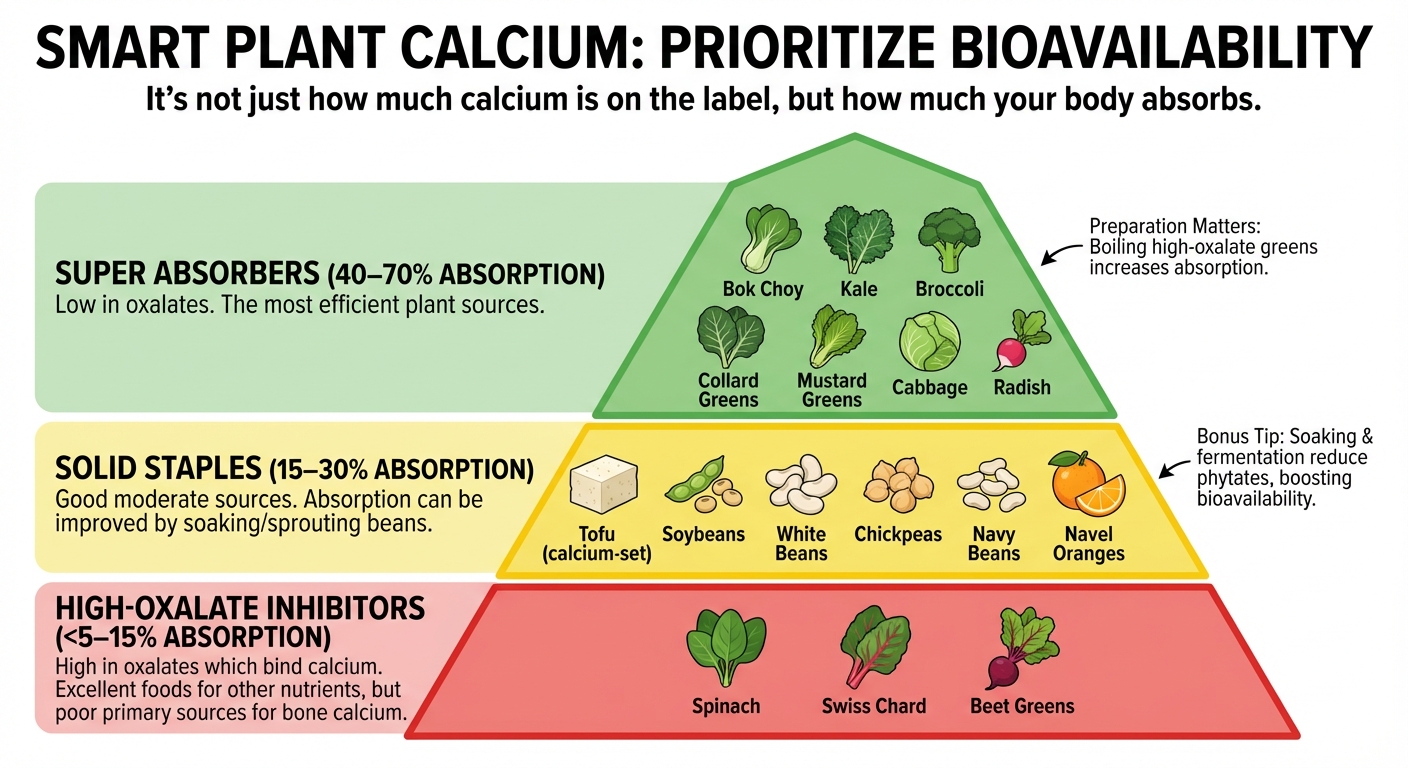
- Phytates and oxalates (legumes, whole grains, nuts, spinach, etc.) bind calcium and reduce bioavailability. High-oxalate foods like spinach absorb only ~5% of calcium, while low-oxalate vegetables like broccoli absorb 47.8%.
However, these effects are substantially reduced with common food-preparation methods and are modest when total calcium intake is adequate.
- Cooking/Boiling: Boiling vegetables can reduce soluble oxalates by 30 to 87%, increasing calcium absorption.
- Soaking/Germination: Soaking cereals can reduce phytates by 17 to 28%, while soaking chickpeas can reduce phytates by more than 50%, increasing absorbed calcium.
- Prebiotic fibres can modestly enhance calcium absorption. For example, supplementation with soluble inulin increased absorption from 21% to 34% in healthy young adults, highlighting how prebiotics can enhance the body’s uptake of calcium.
- Gut health influences both calcium absorption and retention. Short-chain fatty acid-producing bacteria enhance colonic calcium uptake.
The Gatekeepers of Absorption
Vitamin D
Vitamin D is a critical regulator of intestinal calcium absorption. The active form, 1,25-dihydroxyvitamin D (calcitriol), binds to gut receptors and promotes transcellular absorption, especially when dietary calcium is low. For example, someone with low vitamin D may absorb 10 to 15% of that, while higher vitamin D levels can increase absorption 30 to 40%, effectively doubling the calcium taken in from the same meal.
Biological and Environmental Determinants
1. Hormones
- Parathyroid Hormone (PTH) responds to low calcium levels by increasing vitamin D activation and absorption.
- Thyroid Hormones: Thyroid hormones: Hyperthyroidism accelerates bone turnover and urinary calcium loss; individuals with elevated thyroid levels may excrete significantly more calcium, often leading to a net negative calcium balance compared to healthy function. Conversely, hypothyroidism may reduce absorption efficiency due to various factors, such as low stomach acid, which impairs the breakdown of calcium for absorption.
- Estrogen maintains vitamin D sensitivity and regulates bone turnover. After menopause, lower estrogen can reduce calcium absorption by 10 to 20%.
2. Age Fractional calcium absorption peaks in infancy (~60%), rises again during puberty to support peak bone mass, is in the 25 to 30% range for young healthy adults, and gradually declines with age due to reduced vitamin D responsiveness and kidney function. Older adults may absorb below 20% from the same foods.
3. Calcium Content Varies with Soil Chemistry and Growing Conditions Crops grown in calcareous, calcium-rich soils tend to accumulate more calcium in their tissues. For example, in southwestern China, plant species growing in high-calcium soils contained significantly more tissue calcium than the same species grown in low-calcium soils. Similarly, broccoli cultivated in calcium-rich solution has been shown to provide around 100 mg of calcium per 100 g, compared with roughly 50 to 80 mg per 100 g when grown in lower-calcium soils, illustrating how growing conditions directly influence food calcium levels.
4. Gastrointestinal Disorders Fat malabsorption, celiac disease, Crohn’s disease, gastric bypass, chronic kidney disease, hypoparathyroidism, and long-term proton pump inhibitor (PPI) use can all impair calcium absorption through reduced gut integrity, altered vitamin D metabolism, or lower stomach acid.
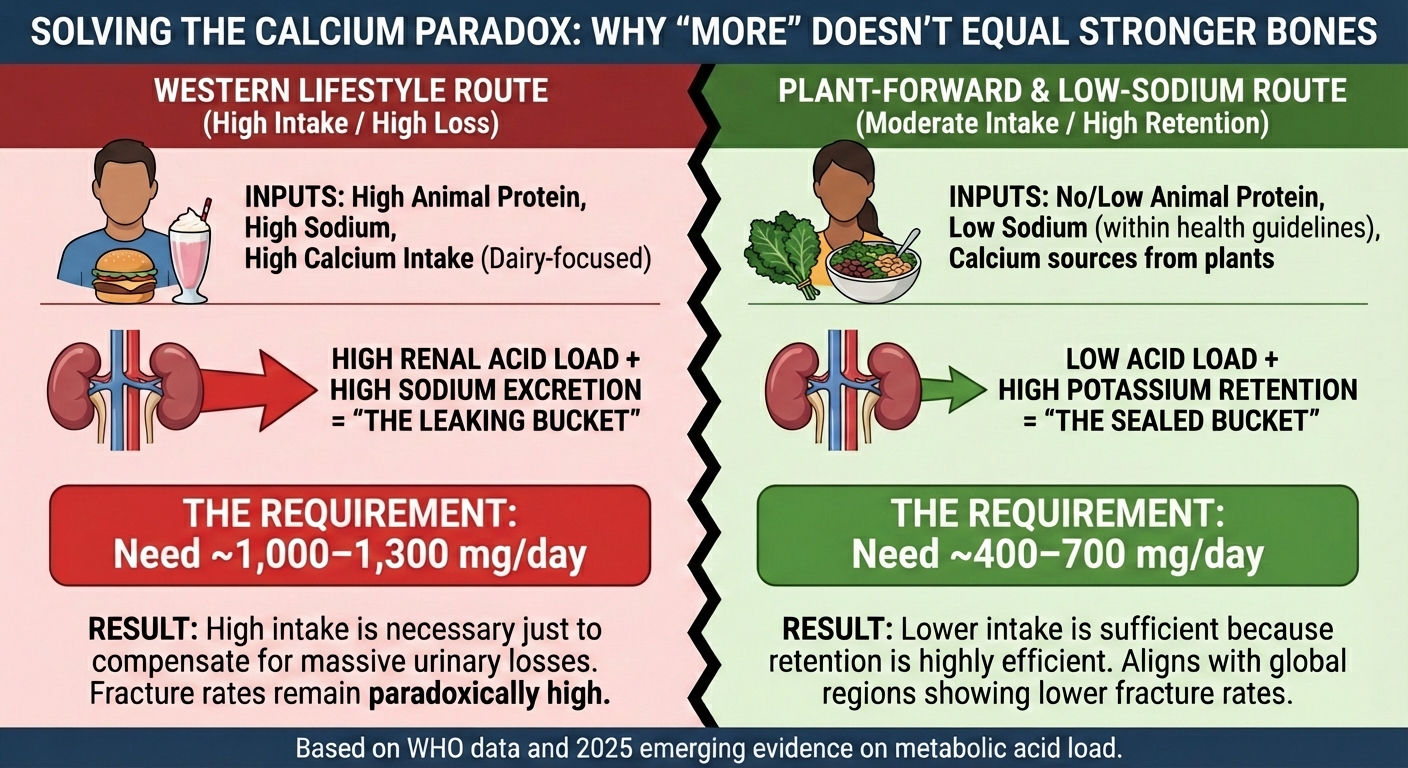
The Global Evidence: The Calcium Paradox
In short, calcium intake alone does not determine skeletal health. Net calcium balance is shaped by the interplay of absorption efficiency and excretion.
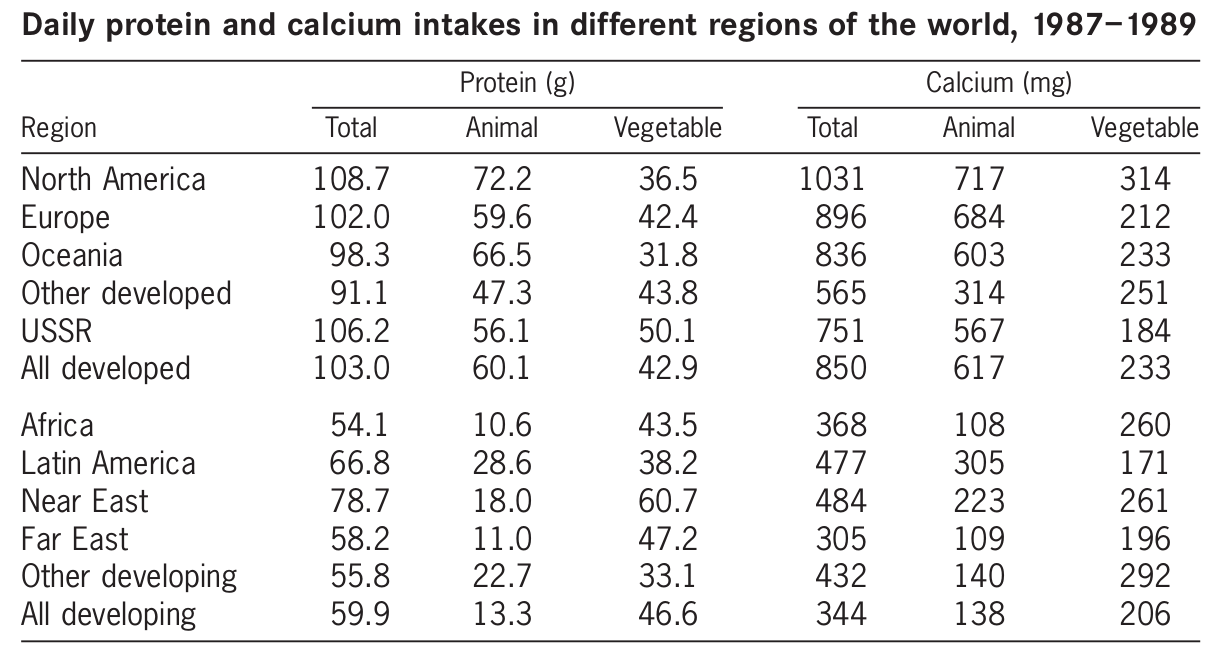
The calcium paradox illustrates this: countries with high calcium intake but also high animal protein intake often have more hip fractures, while nations with moderate calcium intake and lower animal protein intake have fewer fractures.
This phenomenon is not a new discovery; it has been acknowledged by global health authorities for decades. As the World Health Organization (WHO) stated in their seminal report on vitamin and mineral requirements, as well as their technical report on diet, nutrition and chronic diseases:
There is no case for global, population-based approaches. A case can be made for targeted approaches with respect to calcium and vitamin D in high-risk subgroups of populations, i.e. those with a high fracture incidence.
Many other publications point to the same conclusion—that hip fracture prevalence (and by implication osteoporosis) is related to affluence and, consequently, to animal protein intake, as Hegsted pointed out, but also, paradoxically, to calcium intake because of the strong correlation between calcium and protein intakes within and between societies.
The report of the Joint FAO/WHO Expert Consultation on Vitamin and Mineral Requirements in Human Nutrition made it clear that the recommendations for calcium intakes were based on long-term (90 days) calcium balance data for adults derived from Australia, Canada, the European Union, the United Kingdom and the United States, and were not necessarily applicable to all countries worldwide. The report also acknowledged that strong evidence was emerging that the requirements for calcium might vary from culture to culture for dietary, genetic, lifestyle and geographical reasons. Therefore, two sets of allowances were recommended: one for countries with low consumption of animal protein, and another based on data from North America and Western Europe.
The calcium paradox exists because calcium requirements are not fixed; they are determined by balance studies, measuring how much calcium you need to eat to match what you lose.
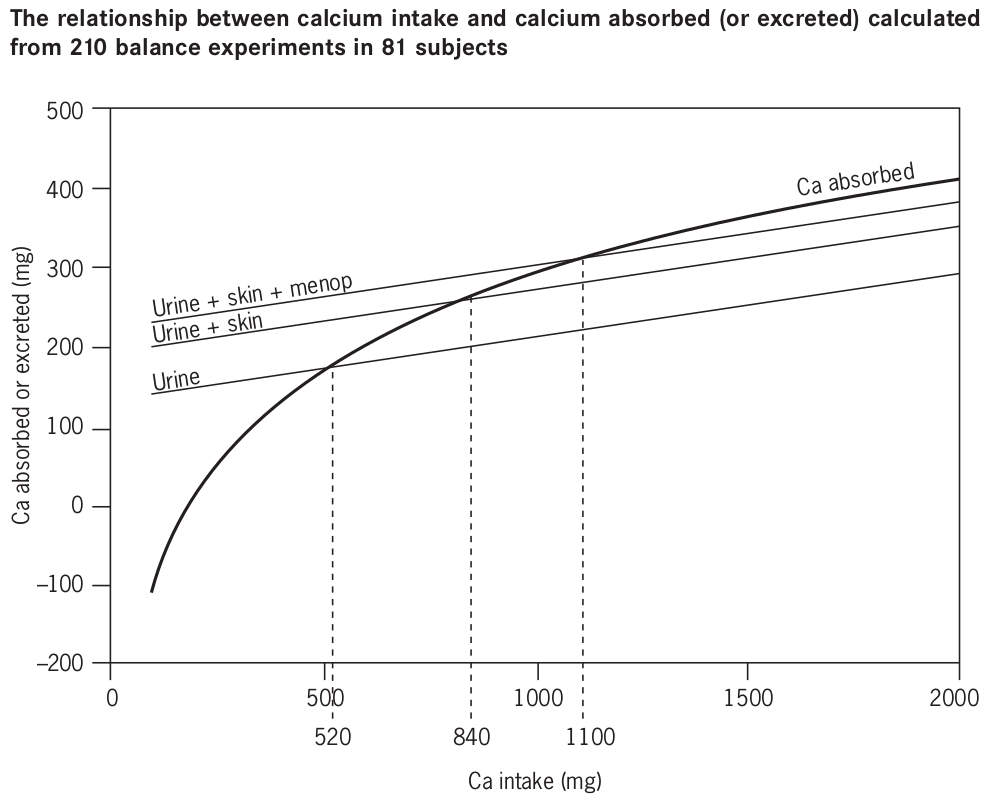
However, this high requirement is not universal. It is a specific result of the Western lifestyle. The World Health Organization (WHO) analyzed how these requirements shift when the leaks-sodium and animal protein-are plugged.
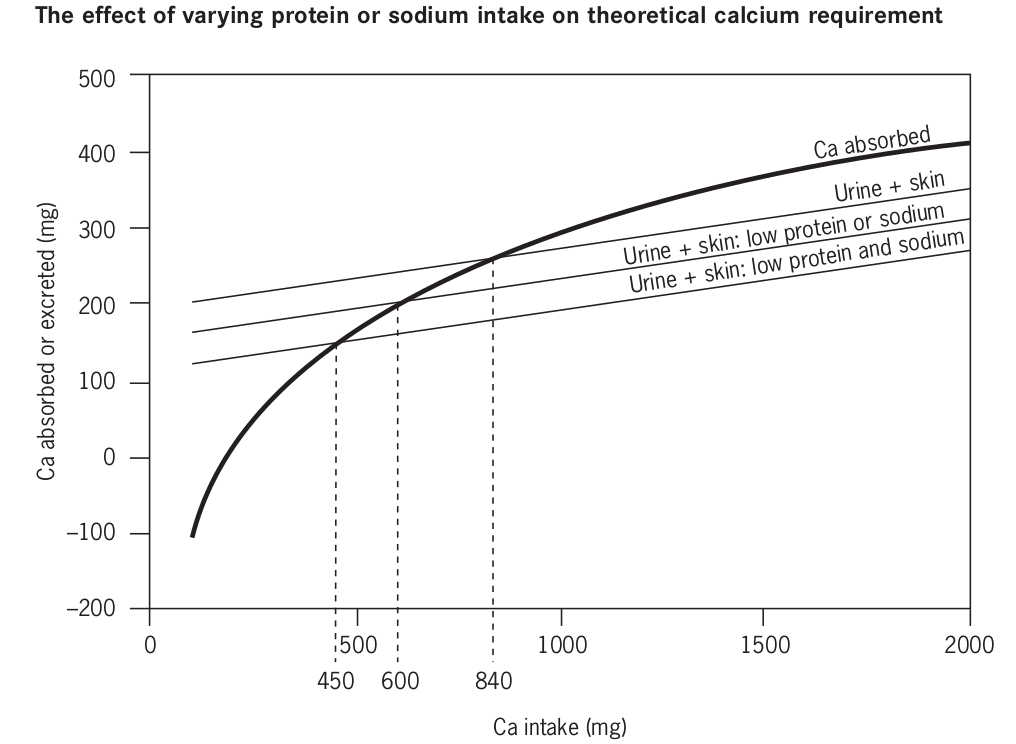
When we apply this model to a diet free of animal protein, like a vegan lifestyle, that also adheres to sodium guidelines, the mathematical requirement shifts further.
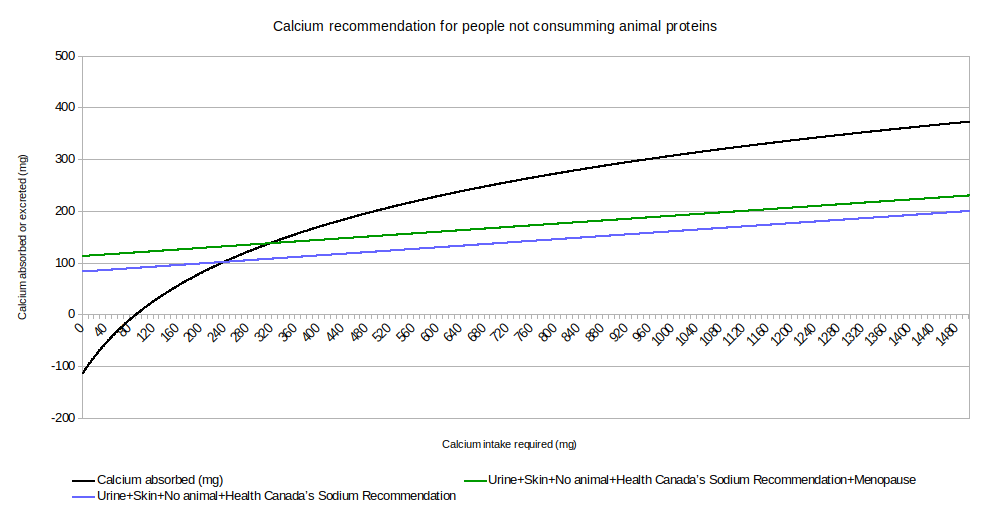
This data solves the Calcium Paradox. The reason North Americans need 1,000+ mg while much of the world stays strong on much less is not genetics; it is the metabolic cost of animal protein and sodium. This is because we are trying to bail a leaking bucket with a larger spoon, rather than fixing the leak.
This underscores that supporting bone health requires a holistic approach, not just meeting a numeric calcium target.
Deficiency Risks
Calcium deficiency can develop when intake, absorption, or retention is insufficient to meet the body’s needs. However, it is crucial to distinguish between physiological requirements and the inflated targets often promoted in Western guidelines. While chronic low calcium status can increase the risk of osteoporosis and fragility fractures, the steep trajectory of bone loss observed in Western populations is not inevitable. High-sodium and high-acid load dietary patterns, characterized by animal protein consumption, act as accelerants, precipitating fractures in aging populations that might otherwise remain asymptomatic in a different dietary context.
Certain populations are naturally more vulnerable, including postmenopausal women and older adults, due to reduced absorption efficiency. Yet, the physiological stress placed on the system by animal protein is universal. Every gram of animal protein generates a fixed acid load that must be buffered, often by calcium. Therefore, while genetics and age play a role in bone density, they do not immunize the body against the calcium-depleting effects of an animal-based diet.
Clinically, early calcium deficiency is often subtle or completely silent, because the body tightly regulates blood calcium by drawing from bone reserves long before serum levels fall. Unlike the dramatic symptoms often listed in scare tactics, such as seizures or heart rhythm abnormalities, which are generally caused by acute medical conditions rather than simple dietary gaps, the primary consequence of long-term dietary inadequacy is gradual osteopenia. This silent reduction in bone mass highlights why the focus must be on lifelong retention, stopping the leak, rather than chasing symptoms with high-dose supplementation.
Although vegans often consume less calcium than omnivores, evidence suggests that the diet itself is not inherently harmful to bone health. A 2025 meta-analysis indicates a higher fracture risk in vegans who fail to meet a minimum calcium threshold. However, this reflects an implementation gap, not a physiological flaw in a diet based on plants. Unlike the omnivorous diet, which relies on a high-intake/high-excretion model, the leaking bucket, a well-planned diet suitable for people who self-identify as vegan offers a low-excretion model that preserves bone density with lower total calcium loads, provided minimum thresholds and Vitamin D adequacy are met. In summary, adequate calcium intake is not a fixed absolute, but a variable dependent on the body's acid load and retention efficiency.
High Intake Risks
Calcium is essential for skeletal, neuromuscular, and cardiovascular function, but intake substantially above typical requirements may carry potential adverse effects, particularly when derived from supplements rather than whole foods.
Although individual tolerance varies, intakes above roughly 1,500 mg/day and especially from supplements or fortified foods are often considered high, and long-term consumption near or beyond the tolerable upper intake levels (UL) warrants a precautionary approach.
Sustained high calcium intake, particularly via supplementation or fortification, may predispose to renal calcification, kidney stones, and impaired renal function. While most stones are composed of calcium and oxalate, the risk is not determined by calcium intake alone. The acid load from animal protein and high sodium intake significantly increases urinary calcium concentration and acidity, creating the optimal environment for oxalates to crystallize. Thus, high calcium intake poses the greatest risk when combined with the typical Western dietary pattern.
There is also concern for cardiovascular effects: studies suggest that persistent elevations in serum calcium, especially from supplements, might correlate with adverse lipid profiles and vascular calcification, potentially contributing to arrhythmias or cardiovascular disease over time.
Recent meta-analytic data indicate that the source of calcium matters. While calcium from dairy products was associated with increased prostate cancer risk, with elevations of 5% per additional 300 mg/day, calcium from plant sources was not associated with cancer risk.
Evidence from observational research also suggests that calcium intake may have a U-shaped association with long-term health outcomes. In a large prospective cohort, individuals with very low dietary calcium intake showed a modestly higher probability of all-cause mortality (HR ≈ 1.22; 95% CI: 1.04–1.42). Conversely, those with the highest intakes exhibited a slightly elevated probability of cancer-related mortality (HR ≈ 1.43; 95% CI: 1.01–2.01), relative to participants with mid-range intakes.
Although these findings do not establish cause and effect, they suggest that both chronic under-consumption and long-term high intake may be associated with less favourable outcomes. These data align with the World Health Organization’s acknowledgment that lower intakes of 400 to 500 mg are not associated with pathological consequences in countries with low fracture rates. Taken together, current evidence tends to support a moderate, food-based calcium intake, using low-dose supplementation only to bridge gaps, while acknowledging that optimal levels likely vary across individuals and contexts.
Supplementation and Safety
The safest strategy is to shift the focus from gross calcium intake to net calcium retention. Evidence suggests that eliminating sources of high renal acid load, like animal proteins and excessive sodium, is more effective for long-term skeletal integrity than simply increasing calcium consumption to offset those losses.
Calcium from whole foods is absorbed more slowly and steadily, and is generally associated with fewer systemic risks than high-dose supplements. While early symptoms such as digestive discomfort or muscle changes can signal excessive intake, longer-term consequences (like kidney stones, vascular calcification, or potential cancer associations) highlight the importance of avoiding unnecessary large supplemental doses.
In addition, while high-dose calcium loading greater than 1000 mg/day via supplements is associated with increased risks, this must not deter appropriate supplementation when dietary intake is low. Small, divided doses, e.g. 200 to 300 mg, used to bridge the gap to a 500 to 700 mg target, are safe. The industry narrative that supplements are dangerous can be a marketing tactic to position dairy as the only safe source; however, vegetables and fortified plant foods offer similar bioavailability without the animal protein acid-load.
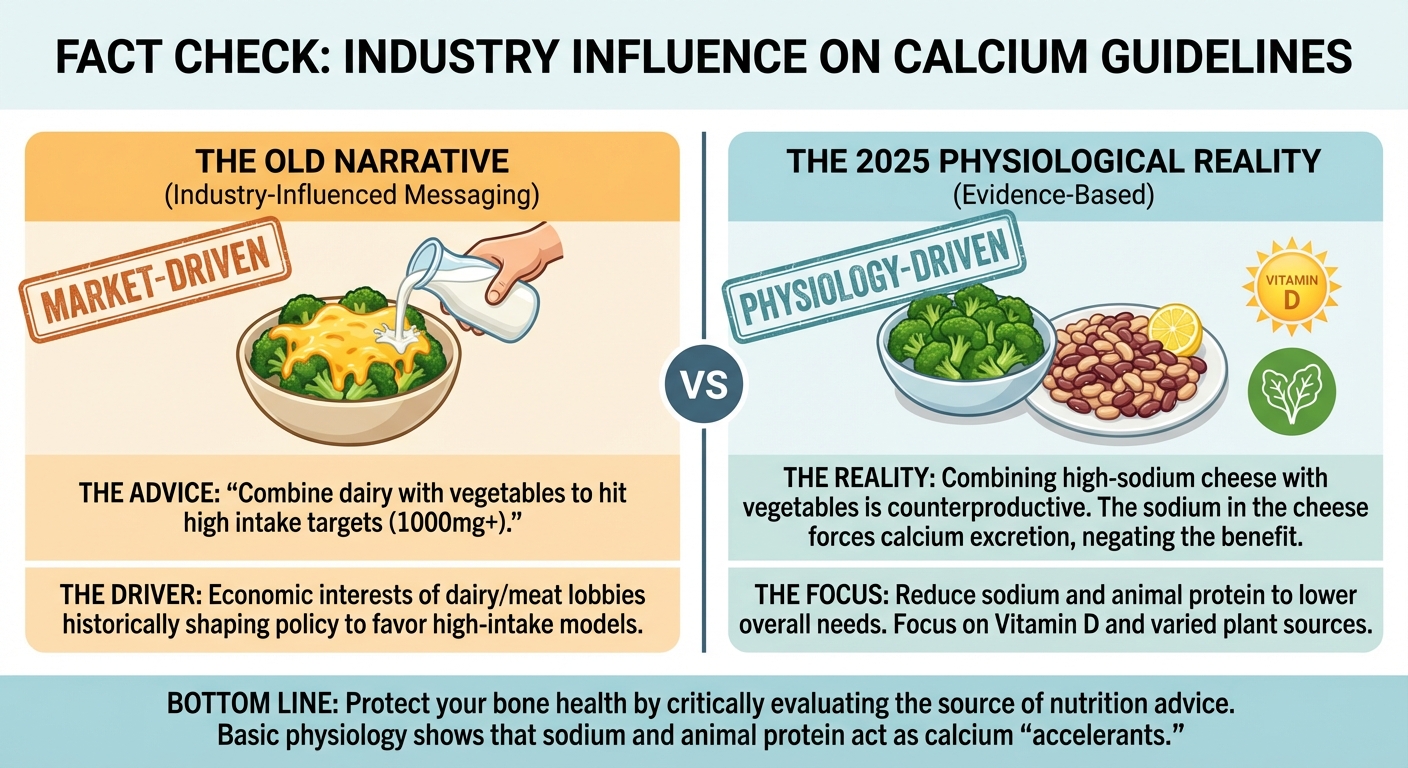
Industry Influence and Public Recommendations
While we now understand the many factors influencing calcium absorption and retention, it’s also clear that public calcium recommendations have been shaped by social, economic, and industry factors, sometimes independently of the underlying science.
Calcium intake guidelines have been shaped not only by evolving science but also by longstanding industry influence. Historically, dairy interests have actively promoted higher recommended calcium intakes and strong dairy messaging in national nutrition guidance. In Canada, the dairy sector has been a powerful economic force, with dairy lobby groups marketing products and historically participating in food‑guide advisory processes, a presence that contributes to a disproportionate emphasis on dairy as a calcium source.
Similarly, extensive documentation of meat and dairy industry lobbying in the U.S. shows repeated efforts to influence federal nutrition recommendations, including earlier versions of the food pyramid and other dietary guidance, illustrating how economic interests can shape public perception of nutrient needs.
Independent documentation of lobbying activities demonstrates that economic interests have historically superseded physiological data in the formulation of national guidelines. The disproportionate emphasis of animal agriculture in Canadian and U.S. policy reflects successful market protection strategies rather than unconflicted analysis of bone metabolism. A good example of this corruption is the infographic below.
A clear divergence exists in global calcium recommendations. North American guidelines, most likely developed in consultation with heavily funded trade groups, recommend 1,000 to 1,300 mg, whereas entities in regions where animal agriculture is less influential tend to be around 500 to 700 mg. This gap cannot be explained by physiology; it is best explained by economics.
Overall, the evidence supports a moderate, food-first approach to meeting calcium needs. We recommend that adults following a vegan lifestyle, and keeping sodium within Health Canada’s limits, aim for at least 400 mg of calcium from whole plant foods daily, using supplements only as needed to bridge the gap. Otherwise, we echo the recommendation of others to aim for 500 to 700 mg/day for the general public and to take into account various lifestyle factors, including but not limited to sodium, protein and alcohol intake, which affects calcium absorption.
Therefore, for the general public, we would encourage instead of trying to increase their calcium intake, to simply adopt a vegan lifestyle and Health Canada’s sodium recommendation. The health benefits will be numerous, and the benefits to the planet and countless living beings are also numerous.
Remaining Uncertainties
Although our understanding of calcium metabolism has grown, several gaps remain:
- Long-term studies in vegans are limited. We still lack large, multi-year RCTs that track fracture outcomes specifically in people following vegan or near-vegan diets.
- Interactions with vitamin D, age, and hormones are not well-mapped in vegans. We extrapolate from general-population research, but the combined effects may differ in a vegan context.
- The gut microbiome’s role is still emerging. Early data show that microbial composition affects calcium absorption and retention, but we don’t yet understand how to translate this into practical guidance.
- Public health guidelines lag behind recent findings. Many recommendations (including Canada’s) still reflect older calcium-centric models and have not fully integrated sodium, protein load, microbiome influences, or supplement-associated risks.
Key Takeaways
- Optimize sources of calcium, particularly from a variety of plant foods.
- Prioritize low-oxalate plant sources of calcium. Regular servings of kale, bok choy, collards, broccoli, and other cruciferous vegetables can safely and significantly boost calcium intake.
- Upper limits do matter, but they are rarely an issue for people eating mostly whole plant foods. The WHO sets the tolerable upper intake at 3,000 mg/day, and it’s nearly impossible to reach that level through unfortified plant foods alone.
- More isn’t better, as very high supplemental intakes raise cardiovascular and mortality risks, while calcium from whole plants is absorbed gradually and safely without the metabolic spikes seen with supplements.
- If supplementing, stay under 500 mg/day, using supplements only to fill dietary gaps. Be mindful that some non-vegan supplements pose contamination risks, e.g. heavy metals in certain marine-derived products.
- Reduce sodium, and the processed foods that contain it, to significantly lower urinary calcium losses and help keep overall calcium needs moderate.
- Take a holistic approach. Real calcium needs are shaped by sodium and protein intake, vitamin D status, gut health, physical activity, and much more, not just a milligram target.
- Question the defaults. Public health guidelines often reflect the economic interests of the industries that sit on their advisory boards. When a recommendation contradicts basic physiology, such as combining calcium with sodium-rich dairy, it is a signal to look for the sponsor. Protecting bone health requires not just eating plants, but critically evaluating the source of your health information.
- Guidelines need to evolve. Public health recommendations must reflect current evidence on sodium reduction, plant-rich diets, vitamin D, microbiome science, and the emerging safety concerns surrounding high-dose supplements.
Below is a table of whole foods, including approximate absorption rates when available. Fortified foods and supplements are not included.
| Food Source | Average Calcium (mg) | Estimated Absorption Rate (%) |
|---|---|---|
| Collards (1 cup, boiled) | 268 | 40-60% |
| Soybeans (1 cup, boiled) | 261 | 20-30% |
| Spinach (1 cup, boiled) | 245 | 5% |
| Mustard greens (1 cup, boiled) | 165 | 50-60% |
| White beans (1 cup, boiled) | 161 | 20-30% |
| Cabbage, Chinese (1 cup, boiled) | 158 | 50-60% |
| Bok Choy (1 cup, boiled) | 158 | 50-55% |
| Figs, dried (10 medium) | 136 | 10-20% |
| Navy beans (1 cup, boiled) | 128 | 20-30% |
| Great northern beans (1 cup, boiled) | 120 | 20-30% |
| Chick peas (1 cup, canned) | 109 | 20-30% |
| Black turtle beans (1 cup, boiled) | 102 | 20-30% |
| Swiss chard (1 cup, boiled) | 102 | 5-15% |
| Kale (1 cup, boiled) | 94 | 50-60% |
| Butternut squash (1 cup, boiled) | 84 | 20-30% |
| Pinto beans (1 cup, boiled) | 79 | 20-30% |
| Sweet potato (1 cup, boiled) | 76 | 20-30% |
| Cabbage, green (1 cup, boiled) | 72 | 60-65% |
| Broccoli (1 cup, boiled) | 62 | 50-60% |
| Barley (1 cup) | 61 | 15-25% |
| Brussels sprouts (8 sprouts) | 60 | 60-64% |
| Navel orange (1 medium) | 60 | 30-40% |
| Green beans (1 cup, boiled) | 55 | 30-40% |
| Raisins (2/3 cup) | 54 | 10-25% |
| Rutabaga (1 cup, boiled, mashed) | 43 | 60-61% |
| Molasses (1 tbsp) | 41 | Unknown |
| Radish (1 cup, raw sliced) | 29 | 72-74% |
| Cauliflower (1 cup, boiled) | 19 | 68-69% |
Infographics
Related articles
Don’t get cracking: How egg lobbies skew research
September 23rd 2020

A review of the scientific evidence on the health risks of dairy products
August 3rd 2019

Alzheimer's disease, dementia and the cholesterol link
November 18th 2022
Methionine: A double-edged sword
April 18th 2022